




 Today we will be discussing about Flaviviridae.
Today we will be discussing about Flaviviridae. -Alphaviruses: Togaviridae
-Flaviviruses: Flaviviridae
~Flaviviridae
-Flavivirus
~Pestivirus : Yellow Fever, Dengue, West Nile
-Hepacivirus : Hepatitis C
Lets talk abt Pestivirus
Natural host(reservoir):Allows amplification of the virus and maintain viremia to allow acquisition by the arthropod.
Host: allows infection, but not necessarily maintain viremia.
Dead-end Host: An host from which infectious agent is not transmitted on.
Properties:

-Spherical enveloped virion, 40-50 nm
-Inner core protein C
-Membrane / matrix protein M
-Envelope with glycoprotein peplomers (E)
-Single linear 11 kb positive sense ssRNA :Infectious mRNA
-3’ polyadenylated tail and 5’ cap
-Cytoplasmic replication (perinuclear)
-Polyprotein from genomic RNA cleaved
-3 structural proteins
-Several non-structural proteins
Now we will talk abt the diseases that are caused by Flaviviridae that is currently troubling the nation now...
Dengue

1. Properties
-Most important arbovirus presently
-Southeast Asia to Americas to Pacific to Africa
-Non-fatal dengue fever (DF)
-Usually fatal dengue haemorrhagic fever (DHF) / dengue shock syndrome (DSS)
-4 distinct serotypes based on neutralisation test.
-DEN-1, DEN-2, DEN-3 and DEN-4
-DEN-2 shows greatest antigenic and genotypic distance from the others
-Protective immunity after infection homotypic
News Update
2007, 1500 cases were reported in the first 19 weeks of 2007.
50% higher than 2006.
Mainly due to Dengue 2, the strain causing 60% of these case.
{kind=link}

2.Dengue Infection Cycle

3.Dengue Fever
 A.
A.-Many infections asymptomatic
-Acute infection resulting in fever, severe headache (frontal), retro-orbital pain, nausea and vomiting
-Severe muscle and bone pain
-Severe arthralgia (joint swelling -mainly back) break bone fever
-Maculopapular rash just before recovery
B.Dengue Haemorrhagic Fever/ Dengue Shock Syndrome
-Prior infection and age key factors in DHF and DSS
-Seldom occurs in individuals above 15 years
-Similar to yellow fever in biphasic nature:
~Initial symptoms similar to DF followed by remission
~Sudden deterioration of patent condition
-Severe prostration, hypotension, circulatory collapse, bleeding and shock
-Bleeding
~Petechiae in skin, mucous membranes (mouth)
~Injection and punction sites
~Gastrointestinal bleeding
~Haemorrhagic pneumonia
-WHO grading:
~Grade I : Fever with non-specific, constitutional symptoms and the only haemorrhagic manifestations being a positive tourniquet test
~Grade II : As for grade I, but with specific haemorrhagic manifestations
~Grade III : Signs of circulatory failure or hypotension
~Grade IV : Profound shock with pulse and blood pressure undetectable
-Pathogenesis
~Not well understood despite intensive study –2 theories
~Virulent strain theory
~Some strains more virulent than others
~Molecular studies show variations in sequences amongst different strains within serotypes
~Early evidence pointed to DEN-2
~Antibody enhancement
~Main theory for DHF / DSS
~Main cell target of DEN: monocytes / macrophages
~Most cases of DHF/DSS had prior infection or infants below 1 year had maternal Ab
~Monkey experiments showed similar enhancement
-Possible cause

~Immune system overreacting
~Sever Acute Respiratory Syndrome
-Transmission - Aedes Mosquito (Female)

-Control:
1.Use of Insecticides
2. Use of Mosquito Screen
3. Removal of Stagnant water
Yellow Fever

1.Properties
-Type species of genus flavivirus
-"flavi" –"yellow" in Latin
-Tropical disease in Latin America and Africa
2.History
-Incubation period: 3-6 days
-Viraemia, infectious, headache, malaise, nausea, lassitude, muscle ache (3 days)
-Flushing of head & neck, conjunctival injection, strawberry tongue
3.Severe Yellow Fever
-Remission after acute yellow fever
-Haemorrhagic, hepatic and renal disease
-Fever, vomiting, abdominal pain, dehydration, prostration
-Haemorrhagic / coffee-ground diathesis (black vomit)
-Bleeding from puncture sites of injections and drip needles
-Jaundice

-Massive haematemesis / haemoptysis / intra-abdominal bleeding
-Renal failure, hypotension, shock
-Virus absent from blood, but antibody titre high –implying autoimmunity may play major role
-Mortality 20-50%
-Survivors suffered extended chronic jaundice before full recovery; hepatic and renal failure may persist
4.Transmission:

5.Control:
- Attenuated Vaccine

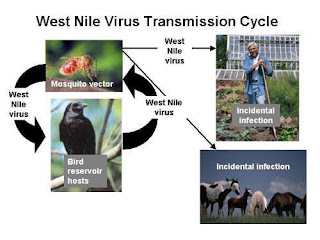
West Nile Fever
1.History
-Originated in Uganda
-Discovered in 1937
-Common in Africa, West Asia, Europe, Middle East
-Spread in US (New York) began in 1999
-Epidemic in US in 2002
2.West Nile Fever
-Mainly mild to no symptoms
-Fever
-Headache, body aches
-Skin rash
-Swollen lymph glands
-Severe symptoms
~Crossing blood-brain barrier
~Encephalitis
~Meningitis
-Mainly in persons above 50 years
3.Transmission:
CONTROL FOR ALL THE DISEASES:
1.Use of Insecticides 
2. Use of Mosquito Screen 
3. Removal of Stagnant water 
The purpose of going through Flavivirdae is because we want to help our peers in their revision and also at the same educate the public on the diseases thats troubling us rite now..